|
Bowen Research & Training
After learning about the Bowen Technique and experiencing how this simple gentle therapy relieved so many of my symptoms, I established Bowen Research & Training Institute primarily to research how the Bowen Technique affects the body. Bowen Therapy is a gentle non-invasive body therapy that seems to bring the autonomic nervous system into balance. I was investigating the effect of the Bowen Technique on the autonomic nervous system (ANS) in patients diagnosed with Fibromyalgia, it was noted that soon after the Bowen therapy, some patients developed flu-like symptoms. Dr. Lida Mattman, who has been culturing cell wall deficient (CWD) organisms from blood for 40 years was contacted to culture specimens from 25 individuals diagnosed with Fibromyalgia Syndrome. She found every sample positive for CWD Borrelia burgdorferi, the causative organism of Lyme disease.
Following this finding 103 seriously ill subjects with a variety of diagnoses were tested and found to be positive for Bb based on Mattman’s Gold Standard Culture method. The conditions included: Fibromyalgia, Osteoarthritis, Mixed Connective Tissue Diseases, Polymyalgia Rheumatica, Ankylosing Spondylitis, Lupus Erythematosus, Palindromic Rheumatism, Chronic Fatigue Syndrome, Multiple Sclerosis, and Amyotrophic Lateral Sclerosis. I was shocked as I was one of that group (my diagnosis at the time was Polymyalgia Rheumatica).
As I tried to come to grips with this finding—that I might have Lyme disease, I thought about my childhood. When did this all start? I grew up in Polk County, Florida and as a kid I spent a lot of time in the woods and had numerous tick bites. I was never diagnosed with any particular malady in my childhood and I never had an EM rash. As a young adult I had bouts of multiple muscle and joint aches and pains but was able to function. I finished high school in 3 years and went on to college at USF and later to medical school at Wake Forrest in Winston Salem, NC. I was very athletic in my youth and won the Florida State Amateur Golf Championship in 1948 and again in 1952. I loved golf but because of my profession never had much time to play.
I recall having periodic muscle and joint aches and pains throughout my life receiving a variety of diagnoses, —Rheumatoid arthritis, Lupus, and Polymyositis Rheumatica. Because of my strong constitution I continued to live a productive life.
For the past six to seven years I have had severe muscle and joint pain and, in retrospect, these symptoms started around the time I saw continuous changes in my number 18 left lower molar. This tooth was extracted January 2000 and contents tested positive for cell wall deficient (CWD) Borrelia burgdorferi (Bb) by the RIBb test and Mattman culture.
During the development of the RIBb test my blood was examined and was positive! I did not believe it. To my surprise the usual negative antibody tests were also all positive including a Lyme Urine Antigen Test (LUAT), which was exceptionally high (over 400). There was no doubt about it. I had Lyme disease and have probably had it since a little girl when I had many tick bites on hunting outings. At that time I was aware that my symptoms were becoming more intense. I had many neurological symptoms—brain fog, short-term memory loss and stiff neck; night sweats, alternating feeling hot and then feeling cold I had extreme hypersensitivity to light, sound and odors. I started wearing dark glasses even inside. I had very little energy, I was easily fatigued, and often had a sore throat. It was very difficult for me to work, I could not last more than and hour or two and even then I was “not worth much”. I began to search for more information on this nonspecific disease and found that I was not atypical. My case was most likely chronic. Finally I was convinced that I did indeed have Lyme disease, so what was I to do about it. It was difficult to find a physician locally to treat my condition. I contacted several known specialists in Lyme disease and one advised me to go on long-term doxycycline, which I did. I also discovered a host of alternative therapies, which I have tried. I have experienced an improvement in many of the symptoms from regular Bowen Therapy treatments. I have tried numerous herbal and nutritional supplements; many have helped and some have not over the long term.
Since discovering that I did indeed have Lyme disease, I have been more or less on continuous antibiotic therapy.
Developing a New Test
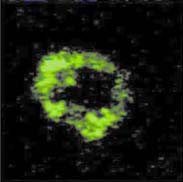
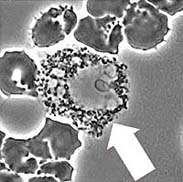
After finding that there were few accurate tests for Borrelia burgdorferi (Bb), my colleague Eleanor Fort, a medical laboratory technologist, with a long history of research involvement in pediatric hematology/oncology and I, at Bowen Research and Training, developed a Rapid identification profile (RIBb©) for this organism. The method uses a fluorescent antibody technique on whole blood and is noteworthy for sensitivity and for the brief time required to complete the test, less than 60 minutes. The accuracy of this method was tested in two other laboratories with identical results. In addition we look at a concentrated suspension of red and white blood cells (rather than a routine blood smear) to identify the co-infections associated with Lyme disease (Ehrlichia in the white blood cell and the parasite Babesia, in the red blood cell. Occasionally we see all three infections in the same individual—Bb, Ehrlichia, and Babesia. All of these patients have definite abnormal peripheral red blood cell morphology. This is noteworthy, as all require different treatment.
The RIBb test has been further refined. We are currently doing Quantative Rapid Identification of Borrelia Burgdorferi Q-RIBb©. This process provides a quantitative titration (serial dilution) method of detecting the antigen in a fluid sample of a subject. The test is considered positive for Lyme disease upon detection of brightly fluorescent antigen-antibody complexes. Antibiotics do not affect the test so it is effective whether or not the person being tested is on antibiotics. When observed in phase contrast, the L-forms can be described morphologically. A preliminary report of the findings is provided within 24 hours of receiving the specimen and the final report includes digital photographs of the findings. This test is useful in evaluating treatment by comparing pre and post serial dilution results.
We have now tested over 3500 specimens, with 500 of these very sick children, from a wide geographical distribution as previously described, and all are positive for cell wall deficient Lyme disease. The primary question is “why are there no negatives?” Does everyone have it? While the majority of our specimens come from individuals who have been diagnosed clinically, we have tested individuals who we “thought” were asymptomatic but were positive for the Bb. An interesting finding is that in 1995, Mattman found forty-three of forty-seven (43/47) patients with chronic diseases to be positive for Lyme disease, while twenty-three of twenty-two (22/23) control cultures were negative. Since 1999, all blood cultures have been positive with Bb, there were no negatives. We believe this indicates the magnitude of the problem. The CDC is now reporting that Lyme disease is more widespread than earlier thought. We believe the problem is not only endemic but may also be reaching epidemic proportions. Early diagnosis is mandatory so that treatment can begin immediately to provide opportunity for cure and prevent chronic Lyme disease.

EXAMPLES OF MISDIAGNOSIS
The following stories of 4 individuals with diagnosis of ALS illustrate how important early diagnosis is.
The first is an individual with a 10-year diagnosis of ALS from whom we received a spinal fluid and blood specimen. The spinal fluid was highly positive for Bb, as was the blood. We reported the findings within a 24-hour period of receiving the specimens only to learn that the individual had died.
The second individual also had a long history of problems identified as ALS. His RIBb test was positive and he was not able to get any physician to treat him for Lyme disease. His health deteriorated and he was admitted to a hospital and was on life support. When his wife was told of his impending death she obtained a court order to have him treated with antibiotic therapy for Lyme disease. He recovered enough to get off life support and was subsequently discharged. He gained weight (32 pounds) and lived eight more months and then died of a heart attack.
The third individual is a 25-year-old golfer on a golf team. He became very ill and was unable to play golf. He was diagnosed with ALS. A family friend knew about our test and sent a blood specimen to be tested for Lyme disease. The results were positive. He was started on appropriate antibiotic therapy and was soon able to resume his golf career. He is now a professional golfer. Having an early diagnosis seems to have made the difference for this young man in living a productive active life.
The FOURTH is a young college student who began having cognitive difficulties and had to drop out of school. He learned about our laboratory and was tested and found to be positive for Lyme disease. After four months on antibiotic he was able to resume his normal active life and is on the deans list and writing classical music.
These examples may shed some light on the importance of early diagnosis and appropriate treatment for Lyme disease. Left untreated the out-come of Lyme disease can result in a chronic debilitating condition and possible death. Are you sure you don’t have Lyme disease? Use RIBb for life.
Dr. Jo Anne Whitaker is President and Director of Research at Bowen Research & Training Institute, Inc. 38541 US Highway 19 North, Palm Harbor, Florida, She can be reached at 727-937-9077 Email JoAnne@bowen.org Web: www.bowen.org
|
|
|